Early this morning, Think Progress (a “progressive” news outlet) posted on Facebook what was meant to be a provocative pull-quote from its latest trans-kid piece by reliable journalist propagandist Zack Ford, “It Takes A Village To Bully A Transgender Kindergartner”:
And what exactly is the “need” of this child? A boy in kindergarten would like to be accepted as “girl”? Well, as a woman, I take offense at any boy who is pretending to share my gender when he quite clearly NEVER can nor ever will. … He is not. He never can be.”
The commenter quoted is, of course, a woman (a bigoted bully, as seen through Ford’s tunnel-vision lens) who questioned the parents’ need to socially transition their 5-year-old child. The child’s transgender status has resulted in a giant kerfuffle as result of the Minnesota school’s dilemma in deciding what to do to accommodate the kindergartner. Zack Ford paints anyone who questions the wisdom of a 5-year-old boy being assured he is really a girl as an ignorant transphobe, a bigot supported only by right-wing conservative groups.

In this post, I’m not going to be writing about the fact that it isn’t just conservatives who question the trans-kid trend (obvious to anyone who reads this blog on a regular basis, or for that matter, the increasing number of blogs by left wing parents, professionals, and feminists. Check out my blogroll). Nor will I be dissecting in detail this “news” article set out as bait on the Think Progress Facebook page to incite the reliable progressive hordes.
Instead, my interest in Ford’s latest bit of Newspeak revolves around the huge number (easily 10-1) of reader comments on that Facebook post, which can be paraphrased as follows:
You stupid bigots! Go read up on the science of gender identity. Gender identity is proven, settled brain science. Little kids KNOW from the time they’re born what sex they are. Plus intersex. No one “chooses” to be transgender, they’re born that way.
I’ve spent thousands of hours marinating in gender dogma and research studies, both pro- and con-, re: “innate gender identity.” So while it’s no surprise to me to see some people spouting as FACT the totally unproven hypothesis that gender identity is set in stone at birth, what does surprise me is the sheer numbers who have bought what, at best, is a tenuous theory, and who have thereby completely shut down even a modicum of critical thinking.
Of course, who can blame well intentioned progressives? They’re fed bittersweet mouthfuls of Innate Gender Identity gruel every single day not only by the media, but even by the President of the United States, who via his Department of Justice, baldly asserts on line 36 of the complaint against the state of North Carolina:
36. Gender identity is innate and external efforts to change a person’s gender identity can be harmful to a person’s health and well-being.

US v. North Carolina
(And it’s not just these few lines. The entire complaint reads like boilerplate trans-activist dogma, and interested readers are urged to take a look at the rest of this document).
This increasingly unchallengeable notion that gender identity, aka “brain sex,” is innate, hard-wired at birth, and thus absolutely unchangeable (despite the efforts of us horrible bigoted parents who are rooting for our kids to commit suicide) means, to the masses who now parrot it like the top graduates of a Maoist Re-Education Camp: Every toddler who claims to be the opposite sex must be agreed with by every adult who comes in contact with the child. Innate gender identity is the ironclad reason why no one is supposed to question the sudden flood of “trans kids” we hear about on a daily basis.
Given the gravity of all this—that little kids are now being ushered aboard a train that will lead inexorably from puberty blockers to cross-sex hormones (with concomitant irreversible changes) in 100% of reported cases–these brain sex/innate gender identity claims can’t just be ignored and dismissed. Not when so many people—more every day—have swallowed them whole.
Here’s the thing. There is some research that supports a role for biological, genetic, or physiological factors in gender dysphoria. And as much as people on “my side” of this argument (the argument being: should children be “transitioned” to the opposite sex on their own say-so?) would like to simply dismiss any and all evidence for biological aspects of things like gender dysphoria, it’s not that simple.
Shunning entire lines of research because we are made uncomfortable by the findings should not be the way of truth seekers. If opening our minds to their claims changes our position, then so be it. As medical historian and intersex-rights activist Alice Dreger says in her book Galileo’s Middle Finger which chronicles (among other things) the chilling effect of activism on scientific inquiry,
[it is] a rare trait in activists: a belief in evidence even when it challenge[s] our political goals.
Human beings, in general, do not appreciate having their cherished ideas challenged. Political viewpoints tend to be set in stone, with any wavering seen by one’s allies as a dangerous and slippery slope. Evidence contrary to the ideological convictions of either side is taken as an existential threat to the fundamental integrity of the position.
For instance, people (like me) who support a woman’s right to abortion often avoid acknowledging the fact that a fetus is not just an amorphous mass of cells, but a proto-human being. Conversely, anti-abortion advocates give short shrift to arguments about a pregnant woman’s agency over her body, and the critical importance of a baby coming into the world to a parent who is ready–and can financially afford–to raise the child.
The battle lines dividing those who support the idea that self/parent/activist-identified “trans” kids should be transitioned as young as possible, vs. those who disagree (like me) are drawn across a long-contested and hardened piece of ground: nature vs. nurture. And the opposing combatants are highly reluctant to give even an inch on the matter.
As you’ll see, this post is going to argue not for a détente or concession of territory, but rather, for a willingness of “my side”—the gender critics–to consider the evidence marshaled by our detractors, and then ponder whether it changes your mind. I’m only going to touch on a few areas of research typically used by the trans activist side; if you’re interested, you’ll want to spend some delving time yourself.
Let me cut to the punchline right now: Speaking for myself, weighing the claims (and the research they base it on) of the activists who want to transition children as early as possible has actually strengthened my conviction that medical transition should be an adults-only decision, if made at all. The only thing I can say I might have shifted my opinion on after endless investigation is this: There may be a very small (it’s always been very small) number of people for whom medical intervention is the only way they can live a happy life. I don’t believe we should prohibit these interventions for such people as adults. I still do not believe, weighing up all the evidence, that we should be tampering with the bodies of young people who may very well grow up to be happy without the expensive, drastic, and irreversible meddling of the gender-soaked medical and psychiatric professions. Instead, as I harp on constantly, let’s celebrate and support gender defiance in young people.
So let’s start with the obvious. [Note to regular readers: The information in the next couple of paragraphs is well known to you, but please stick with me, because I’m going to cover some research I haven’t formerly written about]. If gender identity is “innate” how come so many gender dysphoric youngsters change their minds?
4thWaveNow is chock-a-block with posts and research studies—as well as personal narratives from formerly trans-identified people who changed their minds, as well as others who experienced and resolved severe gender dysphoria in childhood—supporting the fact that many children outgrow their dysphoria and grow up to be adults happy to have bodies and brains that have not been tampered with by the medical and psychiatric professions. A 2008 meta-study by Korte et al sums it up:
Multiple longitudinal studies provide evidence that gender-atypical behavior in childhood often leads to a homosexual orientation in adulthood, but only in 2.5% to 20% of cases to a persistent gender identity disorder. Even among children who manifest a major degree of discomfort with their own sex, including an aversion to their own genitalia (GID in the strict sense), only a minority go on to an irreversible development of transsexualism.
Because so many trans activists claim that intensity of discomfort with one’s body parts is some irrefutable sign of “true transgender,” or that prior researchers didn’t adequately differentiate between “true trans kids” and the merely “gender nonconforming,” I’m going to emphasize this bit of the above quote:
“even among children who manifest a major degree of discomfort with their own sex, including an aversion to their own genitalia.”
Even WPATH—World Professional Association for Transgender Health—whose clinician-activists spend a good deal of time promoting younger and younger ages for “transition,” acknowledges on page 12 of its Standards of Care that most trans-identified kids grow out of it:
In most children, gender dysphoria will disappear before, or early in, puberty.
An earlier online version of the WPATH SOC-7 cited specific numbers—greater than 80%–and included research citations, but this more specific information, oddly enough, has disappeared. But this 2014 study remembers:
…as the World Professional Association for Transgender Health notes in their latest Standards of Care, gender dysphoria in childhood does not inevitably continue into adulthood, and only 6 to 23 percent of boys and 12 to 27 percent of girls treated in gender clinics showed persistence of their gender dysphoria into adulthood.
Ok. So most kids grow out of gender dysphoria. But that fact doesn’t by itself dispense with biological evidence for gender dysphoria, whether or not it persists.
Traditionally, feminists have staked their claim on the “nurture” side of the “gender identity is innate” argument, with little acknowledgement of the findings in biology and neuroscience that hint at any real difference between male and female brain physiology. And there is plenty of hard science bolstering this nurture-based stance: recent MRI studies have mostly corroborated the view that male/female brains are more alike than different, which leads to the conclusion that sex-role stereotyped behaviors are primarily the result of socialization, as Cordelia Fine laid out in her “Delusions of Gender.”

Trans activists and the clinicians who (let’s face it) follow their lead obviously point to other studies of adult transgender people which support the idea that their brains are hard-wired to be closer to the sex they “identify” with. Some of these studies do offer some evidence for sex differentiation in the brain. But imaging studies of adult brains are pretty much impossible to control, because all adults have had life experiences and social influences (not to mention possible cross-sex hormone treatments in some cases) which, owing to neuroplasticity, will of course have an impact on brain structure.
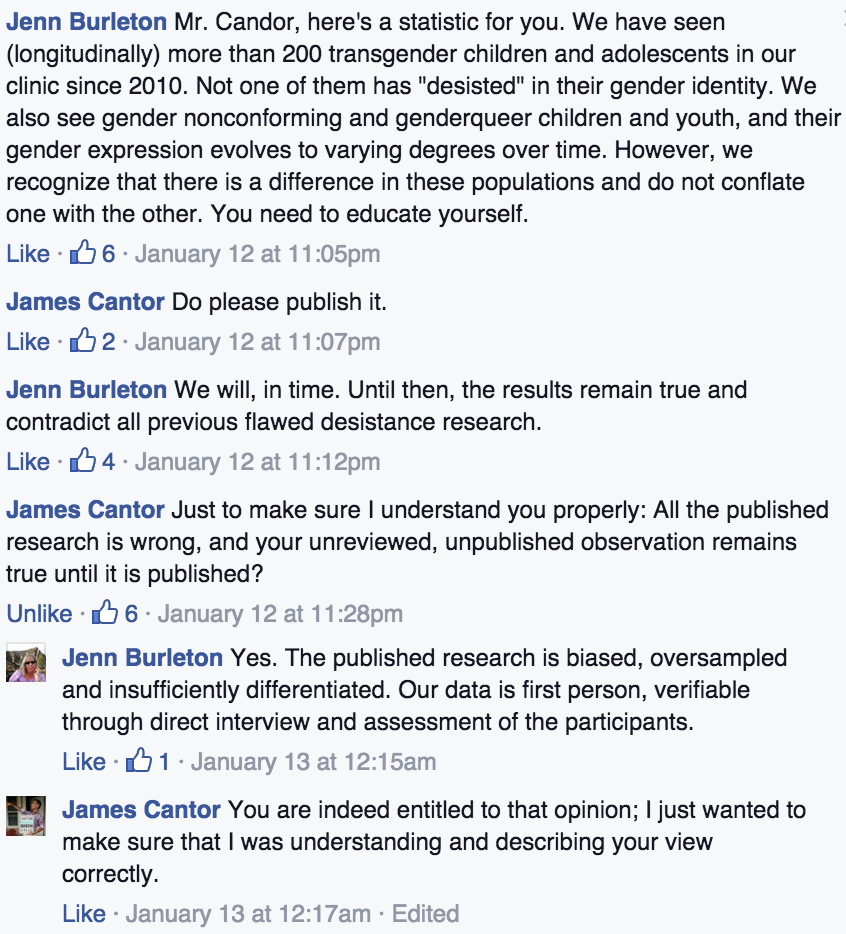
But even in the (primarily MRI) studies of adult brains that are better executed and controlled, it turns out the fundamental difference in these studied brains is not so much a matter of the subjects’ gender identity but of their sexual preference, as sexologist James Cantor draws attention to in a blog post surveying research studies frequently cited to prove a transsexual brain:
In Scientific American Mind, journalist Francine Russo takes on a fascinating research question: “Is there something unique about the transgender brain?” she reviews some of the relevant brain research on transsexuals and concludes that transgenderism is indeed a phenomenon of the brain. Although I agree with Russo that transgenderism is a phenomenon of the brain, I believe Russo over-focused on gender identity, which led her away from the better explanation of the data:
These brain scans don’t reflect gender identity, they reflect sexual orientation.
Cantor’s post, Russo’s Scientific American piece, and the cited research studies are all well worth reading.
There is some other research I find compelling: studies of prenatal hormone levels—specifically, testosterone—and their influence on sex-stereotyped behaviors and other characteristics in children.
A couple of years ago, Brynn Tannehill, a trans activist-journalist, posted a list of what Tannehill obviously considered to be airtight studies, many of them revolving around prenatal hormones, in support of innate gender identity . But are they airtight?
First, Tannehill conveniently neglects to mention that many of the cited studies (surprise, surprise) also show a link between prenatal testosterone levels and rate of homosexuality—in other words, hormone levels may have some impact on same-sex attraction.
But, more importantly, it turns out that several of the researchers linked by Tannehill have shown that the impact of hormones on both sexual identity and gender identity, while existing, is small. For example, Melissa Hines, in a 2006 paper, “Prenatal testosterone and gender-related behaviour, looked at several studies and concluded that
Levels of prenatal testosterone predict levels of sex-typed postnatal childhood play behavior.
Like what kinds of play behavior?
Research on girls and women with CAH has provided some support for the hypothesized influence of testosterone on human behavioural development. Girls with CAH show increased male-typical play behaviour, including increased preferences for toys that are usually chosen by boys, such as vehicles and weapons, increased preferences for boys as playmates and increased interest in rough-and-tumble play.
Does this preference for rough-and-tumble, stereotypical “boy” play mean these kids are transgender?
Although there are fewer studies relating prenatal testosterone levels to postnatal sexual orientation and core gender identity, there is also some evidence, particularly from women with CAH or CAIS, that testosterone influences these psychosexual outcomes as well. However, these influences are substantially smaller than those on childhood play behaviour.
Prenatal testosterone levels are only a small factor in later sexual orientation and gender identity. What they are more predictive of is –wait for it—preference for non-sex-stereotyped activities! In other words: gender nonconformity (or my preferred term: gender defiance).
So some children play with stereotypically opposite-sex toys, prefer the hairstyles and activities of the opposite sex, and prefer the company of children of the opposite sex. Is it possible these preferences are at least partially “hard-wired” due to the effect of androgens on their brains? Sure. Does it follow that this means they are the opposite sex? Of course not. Nor does it necessarily mean they will grow up to be same-sex attracted, either (as I’m sure many heterosexual women who were tomboys can attest).
Let’s put a finer point on it: while some studies show that prenatal hormone levels could contribute to sex-stereotyped differences in human behaviors and, yes, sense of self, acknowledging these differences doesn’t lead to the conclusion that trans activists reach: If a child is born with a set of proclivities and tendencies more typical of the opposite sex, this means they ARE the opposite sex and medical and chemical alteration of the body is fully justified and should be pursued as soon as possible.
What else does biological or genetic research show? In an earlier post, I argued that the only way to even begin to prove an innate male or female brain would be to scan a huge number of identical-twin newborns (before they had a chance to have any “nurture” influence—i.e., no social experiences), separate the twins at birth, then compare those brains later when the children grew up, some of whom would no doubt decide to undergo transition to the opposite sex.
For ethical reasons, this sort of research would be pretty much impossible (you can’t forcibly separate twins at birth and raise them separately, and you can’t control how kids are raised by dictating to parents how to raise them, even if you could). But an international team of researchers has looked at twins and the prevalence of gender dysphoria/transsexualism in a meta-analysis published in 2012, “Gender Identity Disorder in Twins: A Review of the Case Report Literature.” (The full study is behind a paywall.)
Using a combination of their own clinic records and an exhaustive search of the literature, they examined a total or 44 twins of which at least one twin had gender identity disorder (GID)—the diagnostic term at the time, since replaced with “gender dysphoria” (GD). Of these, 23 were identical (monozygotic/MZ). The remainder were fraternal (dizygotic/DZ).
What were their findings?
Nine (39.1%) of the 23 MZ [identical] female and male twins were found to be concordant for GID. In contrast, none of the 21 DZ [fraternal] twin pairs were concordant for GID.
This was a statistically significant difference, leading to the conclusion that “there is a role for genetic factors in the development of GID.” That difference in rate of gender dysphoria in identical twins matters. But let’s not lose sight of the fact that it was still a minority (39.1%) of identical twins who were both gender dysphoric.

In their discussion of their findings, the authors (like all truth-seeking scientists who submit their work to peer review) acknowledge that reality is nuanced:
The higher concordance for GID in MZ than in DZ twins is consistent with a genetic influence on its genesis although shared and nonshared environmental factors cannot be ruled out. Indeed, from these case reports, very little is known about the “equal environments assumption,” that is, the assumption that MZ twins are not treated more similarly than DZ twins in ways that might affect their gender identity.
In other words—“nature” appears to be a factor, but we can’t rule out nurture. ”Influence” is not causality.
And of even greater interest: In the penultimate paragraph of the discussion, we find this gem:
In the studies on genetics and sexual orientation, a higher concordance for homosexuality has been found in MZ versus vs. DZ twins. Using family methodology, there is also evidence for genetic influences [38]. In the reviewed case studies of twins with GID, from those whose sexual orientation is known, all, with the exception of Green [25], were attracted to their biological sex and nearly 50% of the non-GID twins were also homosexual, reflecting a higher percentage than found in the general population [39]. In all the cases reported to be concordant for GID, there was also concordance for sexual orientation.
Here we have it again. As Cantor noted, as I have noted, as the Dutch pioneers of pediatric transition have noted, this study finds—as nearly every study over decades has found: Whatever the precise contributions of nature v. nurture that leads to gender dysphoria or opposite-sex identification, a huge majority (if not 100%) of the studied individuals exhibit same-sex attraction by adolescence or adulthood.
I’ll hammer it home again: The constantly repeated refrain by trans activists that gender identity has “nothing to do with sexual orientation” is directly refuted in every study, as well as many of the personal accounts by trans-identified people splattered all over the media.
So, what have we learned from looking at a few studies aiming to tease apart the nature-nurture question about gender dysphoria/opposite-sex identification?
- there is sparse evidence of an innate male or female brain, and what differences there may be are mitigated and influenced by later life experiences. If anything, brain differences seem to indicate variations in sexual preference, not intrinsic gender identity; and
- prenatal hormones—specifically, testosterone—have an effect, on….gender nonconforming behaviors in childhood. They have a contributing, but minor, effect on later homosexuality and gender identity; and
- in general, there is evidence for both biological and non-biological (environmental-social) contributions to the development of gender dysphoria.
For me, it all boils down to this: Nature v. nurture is a false dichotomy. We are all the result of our genetic inheritance, hormonal influences, and how we were brought up and continue to live—which also includes both post-natal physiological influences (e.g., the various chemicals we imbibe in our hyper-industrialized world in addition to drugs and hormones we deliberately take in), as well as what we learn and experience over the course of our lifetimes.
In the end, the squabbling over nature v. nurture is a non-issue. What matters is protecting kids from the—however well intentioned—meddling of adults in children’s bodily and psychological integrity. Whatever the relative contributions of nature and nurture to a child’s sense of self and ultimate decisions, adults should protect children from undergoing interventions that close off future possibilities.
Proponents of medical transition for children are not champions of gender nonconformity. If they were, as I’ve said many times, they would be celebrating it in children and instead of agreeing with the magical thinking of a child that this means they are “born in the wrong body,” they’d be helping these kids realize they are wonderful and unique examples of their natal sex. A healthy, fully functioning body attached to a brain is an integrated whole with that brain. It is an existential reality, no more “wrong” than the body of a person who demonstrates more sex-stereotyped typicality. By promoting the view that research evidence pointing to certain sex-stereotyped behaviors as having a biological component (however small) means kids’ bodies can be “wrong,” they are using science to limit the possibilities for children.
Puberty blockers, cross sex hormones, and surgeries for children and young people permanently limit their options. Options like: sexual experiences in an unaltered, non-surgically-tinkered-with body. Options like: Figuring out your sexual orientation, especially if you’re gay or lesbian and won’t, on average, come to terms with that fully until early adulthood. Options like: Being a role model for other kids that boys and girls can be and do or be anything, regardless of whether they fit into sex-stereotyped-typical behaviors and appearances.
Yes, a person who later decides to “transition,” who undergoes hormone treatments or surgeries after puberty may not “pass” as well as a someone who had natural puberty curtailed (and was incidentally permanently sterilized in the process). But the Cult of Passing as the opposite sex should be challenged—especially since those same trans activists who worry so much about “passing” (in perhaps their most obvious self-undermining argument) want us to also believe (for instance) that a “penis can be female.” To play Devil’s Advocate with the trans activists, if a boy’s penis can be female, you have no business promoting medical transition for anyone’s child.
Puberty blocking is not a benign intervention. While I’ll grant that, if stopped in time, GnRh agonists are “reversible” (as in, they will not prevent natural puberty), the psychological and neurological effects of delaying natural puberty cannot be seen by any thinking person as “fully reversible.” Neither is social transition “fully reversible,” for that matter. You can’t “reverse” a childhood spent cementing the idea that biological sex can be changed by a society bent on denying the existential reality of sexual dimorphism. You can’t “reverse” a message, repeated over and over to a child by trusted adults that there is something fundamentally wrong with his or her body that must be corrected.
Regarding nature-v-nurture? Here’s what I’d say to my fellow kid transition critics: Don’t dismiss the stuff from the “nature” side because you’ve pre-decided that any science supporting an innate contribution to gender dysphoria is a priori bunk and it’s all nurture/socialization.
In my opinion, taking seriously the dogma of the other side, examining it closely, and then coming to well-thought-out, nuanced conclusions is a much stronger place to operate from than dismissing out of hand any kernel of truth “they” might be obsessing over. That’s not truth seeking; that’s just being close-minded in service of an impenetrable ideology.
Nature-nurture—it’s both. Just like our thought-generating brains are indivisible from the bodies they’re a part of.
Your thoughts?




































{kind=link}